To
the idiot fact checker censors you might can this from here but you cannot
remove it from my blog assholes….
Everything
in this article is taken from this site:
As well as my own personal thoughts
on the matter….MY comments will be in italics – not sure if FB will paste that
in so I will begin with *** as well – my blog will have all the proper
commenting though…
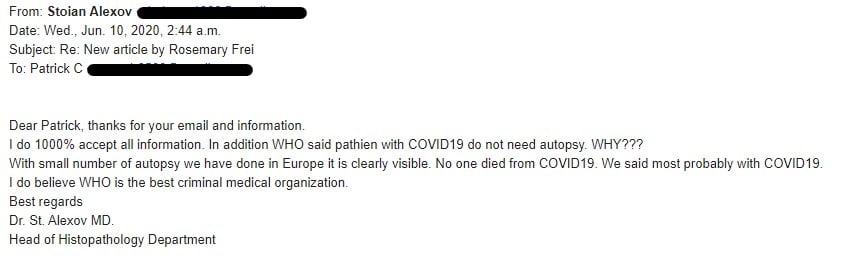
“No
One Has Died from the Coronavirus”
Important
revelations shared by Dr Stoian Alexov, President of the Bulgarian Pathology
Association
**We
all know the Covid-19 numbers are WRONG – yet the mainstream media keeps
shoving them down our throats. So many whistleblowers have come forward with
hidden camera video to PROVE exactly what this website article is saying…. But
the censors keep removing it… labelling it fake or false…. As if Fauci (and I
hesitate to call him a doctor)… is the ONLY reliable source on Covid-19 – why is
that? It is HIS research – he paid to produce it…..
“”Another
stunning revelation from Bulgarian Pathology Association (BPA) president Dr.
Alexov is that he believes
it’s currently “impossible” to create a vaccine against the virus.””
**It is impossible to create a vaccine for
something that does not truly exist…
Novel-coronavirus-specific antibodies are supposedly the basis for the
expensive serology test kits being used in many countries (some of
which have been found to be unacceptably inaccurate).
** We all know that testing in the USA has proved to be inaccurate….
Many “contaminated” testing kits have been found all across the USA thus there
is absolutely no possible way to determine exactly HOW many people actually
have this or how many have truly died from it…
And they’re purportedly key to the immunity certificates coveted
by Bill Gates that
are about to go into widespread use — in the form of the COVI-PASS — in 15 countries including the UK, US,
and Canada.
**
This is what it is all about – it boils down to forced vaccines which will
contain an RFID chip to force us to comply with this immunity certification
bullshit
Among the major bombshells Dr. Alexov dropped is that the
leaders of the May 8 ESP webinar said no novel-coronavirus-specific antibodies have been found.
The body forms antibodies specific to pathogens it encounters.
These specific antibodies are known as monoclonal antibodies and are a key tool
in pathology. This is done via immunohistochemistry,
which involves tagging antibodies with colours and then coating the biopsy- or
autopsy-tissue slides with them. After giving the antibodies time to bind to
the pathogens they’re specific for, the pathologists can look at the slides
under a microscope and see the specific places where the coloured antibodies —
and therefore the pathogens they’re bound to – are located.
**
No specific anti bodies for novel corona virus --- s EVERY test they have ever
done on every person cannot tell if a person has this or if this virus even
exists….
Therefore, in the absence of monoclonal antibodies to the
novel coronavirus, pathologists cannot verify whether SARS-CoV-2 is present in
the body, or whether the diseases and deaths attributed to it indeed were
caused by the virus rather than by something else.
** Since there is no way to detect
antibodies – there is absolutely no way to determine WHAT the person died from…
THUS every number the mainstream media is showing is FALSE and cannot be relied
on as accurate…
In quite a few cases, we have also found that the current
corona infection has nothing whatsoever to do with the fatal outcome because
other causes of death are present, for example, a brain hemorrhage or a heart attack […]
[COVID-19 is] not particularly dangerous viral disease […] All speculation
about individual deaths that have not been expertly examined only fuel anxiety.”
** Their research has shown that this virus is NOT deadly – does NOT
cause death and the media hype IS the problem….
These postulates are scientific steps used to prove whether a virus
exists and has a one-to-one relationship with a specific disease. We showed
that to date no one has proven SARS-CoV-2 causes a discrete illness matching
the characteristics of all the people who ostensibly died from COVID-19. Nor
has the virus has been isolated, reproduced and then shown to cause this
discrete illness.
** Their research has proven that this virus doesn’t even have
consistent characteristics…. Meaning each person is reacting fairly differently
to it…. Meaning there is a good chance that each person has something totally
different….
In addition, in a June 27 Off-Guardian article two
more journalists, Torsten Engelbrecht and Konstantin Demeter, added to the
evidence that “the existence of SARS-CoV-2
RNA is based on faith, not fact.”
The pair also confirmed “there is no scientific proof that those RNA sequences [deemed to
match that of the novel coronavirus] are the causative agent of what is called
COVID-19.”
Dr.
Alexov stated in the May 13 interview that:
the
main conclusion [of those of us who participated in the May 8 webinar] was that
the autopsies that were conducted in Germany, Italy, Spain, France and Sweden
do not show that the virus is deadly.”
He
added that:
What
all of the pathologists said is that there’s no one who has died from the
coronavirus. I will repeat that: no one has died from the coronavirus.”
Dr.
Alexov also observed there is no proof from autopsies that anyone deemed to
have been infected with the novel coronavirus died only from an inflammatory
reaction sparked by the virus (presenting as interstitial pneumonia) rather
than from other potentially fatal diseases.
Another
revelation of his is that:
“We
need to see exactly how the law will deal with immunization and that vaccine
that we’re all talking about, because I’m certain it’s [currently] not possible
to create a vaccine against COVID. I’m not sure what exactly Bill Gates is
doing with his laboratories – is it really a vaccine he’s producing, or
something else?”
**
These are scientists with far more experience than Fauci….They HAVE performed
autopsies on some of those who have died supposedly from Covid-19 and found NO
proof the virus even exists….
Dr.
Alexov therefore asserted that:
the
WHO is creating worldwide chaos, with no real facts behind what they’re
saying.”
Among
the myriad ways the WHO is creating that chaos is by prohibiting almost all
autopsies of people deemed to have died from COVID-19. As a result, reported
Dr. Alexov, by May 13 only three such autopsies had been conducted in Bulgaria.
Also, the WHO is dictating that everyone said to be infected
with the novel coronavirus who subsequently dies must have their deaths
attributed to COVID-19.
“That’s quite stressful for us,
and for me in particular, because we have protocols and procedures which we
need to use,” he told Dr. Katsarov. “…And another pathologist 100 years from now is going to say,
‘Hey, those pathologists didn’t know what they were doing [when they said the
cause of death was COVID-19]!’ So we need to be really strict with our
diagnoses, because they could be proven [or disproven], and they could be
checked again later.”
**
IF this was a real thing WHY would the World Health Organization be PREVENTING
autopsies to study this???? We NEED autopsies to determine precise details and
facts…. So WHY are they preventing these from being performed???? Even in 1918
during the Spanish Flu we did autopsies!!! So why not during THIS pandemic?????
How will we EVER now the truth without such things???
(He added that autopsies could have helped confirm or disprove the
theory that many of the people deemed to have died of COVID-19 in Italy had
previously received the H1N1 flu vaccine. Because, as he noted, the vaccine
suppresses adults’ immune systems and therefore may have been a significant
contributor to their deaths by making them much more susceptible to infection.)
**
Their research has found a link between this illness and the H1N1 vaccine… but
they are NOT being permitted to research it further…. WHY NOT??? My own
personal issue – in December 2019 I received the yearly flu vaccine and within
7 days was damn near on my deathbed sick. I did NOT go to the hospital though –
I treated it the old fashioned way, the way I always treat my yearly bronchitis…..So,
if they have evidence there is a link between this so called illness and a
vaccine shouldn’t we research this and find out for sure??? Why is the WHO
preventing this???
They
also observed these diseases are being exacerbated by the fear and chaos
surrounding COVID-19.
We
know that stress significantly suppresses the immune system, so I can really
claim 200% that all the chronic diseases will be more severe and more acute per
se. Specifically in situ carcinoma – over 50% of these are going to become more
invasive […] So I will say that this epidemic isn’t so much an epidemic of the
virus, it’s an epidemic of giving people a lot of fear and stress.”
**
The WHO and our experts are literally MAKING us sick on purpose… WHY???
{kind=link}
**
In he FEW autopsies he was able to perform NO a single one died of Covid-19 –
so WHY then are so many deaths being labelled as Covid deaths and buried
without an autopsy??? Don’t YOU ant to know what the hell is going on????
What is a coronavirus?
Coronaviruses (CoV) are a large family of viruses that cause illness ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS-CoV). A novel coronavirus (nCoV) is a new strain that has not been previously identified in humans.
Coronaviruses (CoV) are a large family of viruses that cause illness ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS-CoV). A novel coronavirus (nCoV) is a new strain that has not been previously identified in humans.
Coronavirus: a type of common virus that infects humans, typically leading to
an upper respiratory infection (URI.) Seven different types of human coronavirus have
been identified. Most people will be infected with at least one type of
coronavirus in their lifetime. The viruses are spread through the air by coughing and sneezing, close personal contact,
touching an object or surface contaminated with the virus and rarely, by fecal
contamination. The illness caused by most coronaviruses usually lasts a short
time and is characterized by runny nose, sore throat, feeling unwell, cough, and fever.
Definition of coronavirus
1: any of a family (Coronaviridae) of large single-stranded RNA viruses that have a lipid envelope
studded with club-shaped spike proteins, infect birds and many mammals
including humans, and include the causative agents of MERS, SARS,
and COVID-19
Clinical Presentation
Coronaviruses
cause acute, mild upper respiratory infection (common cold).
Structure
Spherical or
pleomorphic enveloped particles containing single-stranded (positive-sense) RNA
associated with a nucleoprotein within a capsid comprised of matrix protein.
The envelope bears club-shaped glycoprotein projections.
Classification
Coronaviruses
(and toroviruses) are classified together on the basis of the crown or
halo-like appearance of the envelope glycoproteins, and on characteristic
features of chemistry and replication. Most human coronaviruses fall into one
of two serotypes: OC43-like and 229E-like.
Multiplication
The virus
enters the host cell, and the uncoated genome is transcribed and translated.
The mRNAs form a unique “nested set” sharing a common 3′ end. New virions form
by budding from host cell membranes.
Pathogenesis
Transmission
is usually via airborne droplets to the nasal mucosa. Virus replicates locally
in cells of the ciliated epithelium, causing cell damage and inflammation.
Host Defenses
The appearance
of antibody in serum and nasal secretions is followed by resolution of the
infection. Immunity wanes within a year or two.
Epidemiology
Incidence
peaks in the winter, taking the form of local epidemics lasting a few weeks or
months. The same serotype may return to an area after several years.
Diagnosis
Colds caused
by coronaviruses cannot be distinguished clinically from other colds in any one
individual. Laboratory diagnosis may be made on the basis of antibody titers in
paired sera. The virus is difficult to isolate. Nucleic acid hybridization
tests (including PCR) are now being introduced.
Control
Treatment of
common colds is symptomatic; no vaccines or specific drugs are available.
Hygiene measures reduce the rate of transmission.
Introduction
Coronaviruses
are found in avian and mammalian species. They resemble each other in
morphology and chemical structure: for example, the coronaviruses of humans and
cattle are antigenically related. There is no evidence, however, that human
coronaviruses can be transmitted by animals. In animals, various coronaviruses
invade many different tissues and cause a variety of diseases, but in humans
they are only proved to cause mild upper respiratory infections, i.e. common
colds. On rare occasions, gastrointestinal coronavirus infection has been
associated with outbreaks of diarrhoea in children, but these enteric viruses
are not well characterized and are not discussed in this chapter.
Clinical
Manifestations
Coronaviruses
invade the respiratory tract via the nose. After an incubation period of about
3 days, they cause the symptoms of a common cold, including nasal obstruction,
sneezing, runny nose, and occasionally cough (Figs. 60-1 and 60-2). The disease resolves
in a few days, during which virus is shed in nasal secretions. There is some
evidence that the respiratory coronaviruses can cause disease of the lower
airways but it is unlikely that this is due to direct invasion. Other
manifestations of disease such as multiple sclerosis have been attributed to
these viruses but the evidence is not clear-cut.

Figure 60-1
Clinical manifestations and pathogenesis
of coronavirus infections.

Figure 60-2
Immunopathogenesis of coronavirus
infections.
Structure
Coronavirus
virions are spherical to pleomorphic enveloped particles (Fig. 60-3). The envelope
is studded with projecting glycoproteins, and surrounds a core consisting of
matrix protein enclosed within which is a single strand of positive-sense RNA
(Mr 6 × 106) associated with nucleoprotein. The
envelope glycoproteins are responsible for attachment to the host cell and also
carry the main antigenic epitopes, particularly the epitopes recognized by
neutralizing antibodies. OC43 also possesses a haemagglutin.

Figure 60-3
Electron micrograph showing human
coronavirus 229E. Bar, 100 mn (Courtesy S.Sikotra, Leicester Royal Infirmary,
Leicester, England.)
Classification
and Antigenic Types
The
coronaviruses were originally grouped into the family Coronaviridae on
the basis of the crown or halo-like appearance given by the
glycoprotein-studded envelope on electron microscopy. This classification has
since been confirmed by unique features of the chemistry and replication of
these viruses. Most human coronaviruses fall into one of two groups: 229E-like
and OC43-like. These differ in both antigenic determinants and culturing
requirements: 229E-like coronaviruses can usually be isolated in human embryonic
fibroblast cultures; OC43-like viruses can be isolated, or adapted to growth,
in suckling mouse brain. There is little antigenic cross-reaction between these
two types. They cause independent epidemics of indistinguishable disease.
Multiplication
It is thought
that human coronaviruses enter cells, predominantly, by specific receptors.
Aminopeptidase-N and a sialic acid-containing receptor have been identified to
act in such a role for 229E and OC43 respectively. After the virus enters the
host cell and uncoats, the genome is transcribed and then translated. A unique
feature of replication is that all the mRNAs form a “nested set” with common 3′
ends; only the unique portions of the 5′ ends are translated. There are 7 mRNAs
produced. The shortest mRNA codes for the nucleoprotein, and the others each
direct the synthesis of a further segment of the genome. The proteins are
assembled at the cell membrane and genomic RNA is incorporated as the mature
particle forms by budding from internal cell membranes.
Pathogenesis
Studies in
both organ cultures and human volunteers show that coronaviruses are extremely
fastidious and grow only in differentiated respiratory epithelial cells.
Infected cells become vacuolated, show damaged cilia, and may form syncytia.
Cell damage triggers the production of inflammatory mediators, which increase
nasal secretion and cause local inflammation and swelling. These responses in
turn stimulate sneezing, obstruct the airway, and raise the temperature of the
mucosa.
Host
Defenses
Although
mucociliary activity is designed to clear the airways of particulate material,
coronaviruses can successfully infect the superficial cells of the ciliated
epithelium. Only about one-third to one-half of infected individuals develop
symptoms, however. Interferon can protect against infection, but its importance
is not known. Because coronavirus infections are common, many individuals have
specific antibodies in their nasal secretions, and these antibodies can protect
against infection. Most of these antibodies are directed against the surface
projections and neutralize the infectivity of the virus. Cell-mediated immunity
and allergy have been little studied, but may play a role.

Figure 60-4
Seasonal incidence of coronavirus
infections.
Epidemiology
The
epidemiology of coronavirus colds has been little studied. Waves of infection
pass through communities during the winter months, and often cause small
outbreaks in families, schools, etc. (Fig. 60-2). Immunity does
not persist, and subjects may be re-infected, sometimes within a year. The
pattern thus differs from that of rhinovirus infections, which peak in the fall
and spring and generally elicit long-lasting immunity. About one in five colds
is due to coronaviruses.
The rate of
transmission of coronavirus infections has not been studied in detail. The
virus is usually transmitted via inhalation of contaminated droplets, but it
may also be transmitted by the hands to the mucosa of the nose or eyes.
Diagnosis
There is no
reliable clinical method to distinguish coronavirus colds from colds caused by rhinoviruses
or less common agents. For research purposes, virus can be cultured from nasal
swabs or washings by inoculating organ cultures of human fetal or nasal
tracheal epithelium. The virus in these cultures is detected by electron
microscopy or other methods. The most useful method for laboratory diagnosis is
to collect paired sera (from the acute and convalescent phases of the disease)
and to test by ELISA for a rise in antibodies against OC43 and 229E. Complement
fixation tests are insensitive; other tests are inconvenient and can be used
only for one serotype. Direct hybridization and polymerase chain reaction tests
for viral nucleic acid have been developed and, particularly with the latter,
are the most sensitive assays currently available for detecting virus .
Control
Although
antiviral therapy has been attempted, the treatment of coronavirus colds
remains symptomatic. The likelihood of transmission can be reduced by
practising hygienic measures. Vaccines are not currently available.
References
2.
Myint
S, Johnstone S, Sanderson G, Simpson H. An evaluation of ‘nested’ RT-PCR
methods for the detection of human coronaviruses 229E and OC43 in clinical
specimens. Mol Cell Probes. 1994;8:357–364. [PMC free article] [PubMed]
3.
Sanchez
CM, Jimenez G, Laviada MD. et al. Antigenic homology among coronaviruses
related to transmissible gastroenteritis virus. Virology. 1990;174:410. [PMC free article] [PubMed]
4.
Schmidt
OW, Allan ID, Cooney MK. et al. Rises in titers of antibody to human
coronaviruses OC43 and 229E in Seattle families during 1975–1979. Am J Epidemiol. 1986;123:862. [PMC free article] [PubMed]
5.
Spaan
W, Cavanagh D, Horzinek MC. Coronaviruses: structure and genome
expression. J Gen Virol. 1988;69:2939. [PubMed]
6.
Tyrrell
DAJ, Cohen S, Schlarb JE. Signs and symptoms in common colds. Epidemiol Infect. 1993;111:143–156. [PMC free article] [PubMed]
Copyright © 1996, The University of Texas
Medical Branch at Galveston.
coronavirus
[ kuh-roh-nuh-vahy-ruh s ]SHOW IPA
noun, plural co·ro·na·vi·rus·es.
any of various RNA-containing spherical viruses
of the family Coronaviridae, including several that cause acute respiratory
illnesses.
Coronavirus
From Wikipedia, the free encyclopedia
This article is about the group of viruses.
For the disease involved in the ongoing COVID-19 pandemic, see Coronavirus
disease 2019. For the virus that causes this disease, see Severe acute respiratory syndrome coronavirus 2. For
the upcoming Indian film, see Coronavirus (film).
|
Orthocoronavirinae
|
|
 |
|
 |
|
|
Illustration of the morphology of
coronaviruses; the club-shaped viral spike peplomers (red) create the
look of a corona surrounding the virion when seen with an electron microscope.
|
|
|
(unranked):
|
|
|
Realm:
|
|
|
Kingdom:
|
|
|
Phylum:
|
|
|
Class:
|
|
|
Order:
|
|
|
Family:
|
|
|
Subfamily:
|
Orthocoronavirinae
|
|
·
Coronavirinae
|
|
Coronaviruses are a group of
related RNA viruses that cause diseases in mammals and birds.
In humans, these viruses cause respiratory
tract infections that can range from mild to lethal. Mild
illnesses include some cases of the common cold (which is also caused by
other viruses, predominantly rhinoviruses), while more lethal varieties can
cause SARS, MERS,
and COVID-19.
Symptoms in other species vary: in chickens, they cause an upper
respiratory tract disease, while in cows and pigs they cause diarrhea. There are as yet no vaccines or antiviral drugs to prevent or treat human
coronavirus infections.
Coronaviruses constitute the subfamily Orthocoronavirinae,
in the family Coronaviridae,
order Nidovirales, and
realm Riboviria.[5][6] They
are enveloped viruses with
a positive-sense
single-stranded RNA genome and a nucleocapsid of helical symmetry.[7] The genome size of coronaviruses ranges from
approximately 26 to 32 kilobases, one of the
largest among RNA viruses.[8] They
have characteristic club-shaped spikes that project from their surface,
which in electron micrographs create
an image reminiscent of the solar corona, from which their name derives.[9]
Contents
·
2History
·
5Origin
Etymology
The name "coronavirus" is derived from
Latin corona,
meaning "crown" or "wreath", itself a borrowing from Greek κορώνη korṓnē,
"garland, wreath".[10][11] The
name was coined by June Almeida and David Tyrrell who
first observed and studied human coronaviruses.[12] The
word was first used in print in 1968 by an informal group of virologists in the
journal Nature to
designate the new family of viruses.[9] The
name refers to the characteristic appearance of virions (the infective form of the virus)
by electron microscopy,
which have a fringe of large, bulbous surface projections creating an image
reminiscent of the solar corona or
halo.[9][12] This morphology is
created by the viral spike peplomers, which
are proteins on the surface of the virus.[13]
History
Coronaviruses were first discovered in the 1930s when an
acute respiratory infection of domesticated chickens was shown to be caused
by infectious bronchitis
virus (IBV).[14] Arthur
Schalk and M.C. Hawn described in 1931 a new respiratory infection
of chickens in North Dakota. The infection of new-born chicks
was characterized by gasping and listlessness. The chicks' mortality rate was
40–90%.[15] Fred
Beaudette and Charles Hudson six years later successfully isolated and
cultivated the infectious bronchitis virus which caused the disease.[16] In
the 1940s, two more animal coronaviruses, mouse hepatitis virus (MHV)
and transmissible
gastroenteritis virus (TGEV), were isolated.[17] It
was not realized at the time that these three different viruses were related.[18]
Human coronaviruses were discovered in the 1960s.[19][20] They
were isolated using two different methods in the United Kingdom and the United
States.[21] E.C.
Kendall, Malcom Byone, and David Tyrrell working
at the Common Cold Unit of
the British
Medical Research Council in 1960 isolated from a boy a
novel common cold virus
B814.[22][23][24] The
virus was not able to be cultivated using standard techniques which had
successfully cultivated rhinoviruses, adenoviruses and other known common cold
viruses. In 1965, Tyrrell and Byone successfully cultivated the novel virus
by serially passing it
through organ culture of human embryonic trachea.[25] The
new cultivating method was introduced to the lab by Bertil Hoorn.[26] The
isolated virus when intranasally inoculated into volunteers caused a cold
and was inactivated by ether which indicated
it had a lipid envelope.[22][27] Around
the same time, Dorothy Hamre[28] and
John Procknow at the University of Chicago isolated
a novel cold virus 229E from medical students, which they grew in kidney tissue culture. The novel virus 229E, like the
virus strain B814, when inoculated into volunteers caused a cold and was
inactivated by ether.[29]

Transmission electron micrograph of organ cultured coronavirus OC43
The two novel strains B814 and 229E were subsequently
imaged by electron microscopy in 1967 by Scottish virologist June Almeida at St. Thomas Hospital in
London.[30][31] Almeida
through electron
microscopy was able to show that B814 and 229E were
morphologically related by their distinctive club-like spikes. Not only were they related with each
other, but they were morphologically related to infectious bronchitis virus
(IBV).[32] A
research group at the National
Institute of Health the same year was able to isolate another
member of this new group of viruses using organ culture and named the virus
strain OC43 (OC for organ culture).[33] Like
B814, 229E, and IBV, the novel cold virus OC43 had distinctive club-like spikes
when observed with the electron microscope.[34][35]
The IBV-like novel cold viruses were soon shown to be
also morphologically related to the mouse hepatitis virus.[17] This
new group of IBV-like viruses came to be known as coronaviruses after their
distinctive morphological appearance.[9] Human coronavirus
229E and human coronavirus
OC43 continued to be studied in subsequent decades.[36][37] The
coronavirus strain B814 was lost. It is not known which present human
coronavirus it was.[38] Other
human coronaviruses have since been identified, including SARS-CoV in
2003, HCoV NL63 in
2004, HCoV HKU1 in
2005, MERS-CoV in 2012, and SARS-CoV-2 in 2019.[39][40] There
have also been a large number of animal coronaviruses identified since the
1960s.[5]
Microbiology
Structure

Cross-sectional model of a coronavirus
Coronaviruses are large, roughly spherical, particles
with bulbous surface projections.[41] The
average diameter of the virus particles is around 125 nm (.125 μm). The diameter of the envelope is 85 nm and
the spikes are 20 nm long. The envelope
of the virus in electron micrographs appears as a distinct pair of
electron-dense shells (shells that are relatively opaque to the electron beam
used to scan the virus particle).[42][43]
The viral envelope consists of a lipid bilayer, in which the membrane (M),
envelope (E) and spike (S) structural
proteins are anchored.[44] The
ratio of E:S:M in the lipid bilayer is approximately 1:20:300.[45] On
average a coronavirus particle has 74 surface spikes.[46] A
subset of coronaviruses (specifically the members of betacoronavirus subgroup A) also have a shorter spike-like
surface protein called hemagglutinin
esterase (HE).[5]
The coronavirus surface spikes are homotrimers of the S protein,
which is composed of an S1 and S2 subunit. The homotrimeric S protein
is a class I fusion
protein which mediates the receptor binding and membrane fusion between
the virus and host cell. The S1 subunit forms the head of the spike and has the
receptor binding domain (RBD). The S2 subunit forms the stem which anchors the
spike in the viral envelope and on protease activation enables fusion. The E
and M protein are important in forming the viral envelope and maintaining its
structural shape.[43]
Inside the envelope, there is the nucleocapsid, which is formed from multiple
copies of the nucleocapsid (N) protein, which are bound to the positive-sense
single-stranded RNA genome in a continuous beads-on-a-string type
conformation.[43][47] The
lipid bilayer envelope, membrane proteins, and nucleocapsid protect the virus
when it is outside the host cell.[48]
Genome

Schematic representation of the genome organization and functional domains
of S protein for SARS-CoV and MERS-CoV
Coronaviruses contain a positive-sense,
single-stranded RNA genome. The genome size for coronaviruses ranges from
26.4 to 31.7 kilobases.[8] The
genome size is one of the largest among RNA viruses. The genome has a 5′ methylated cap and a 3′ polyadenylated tail.[43]
The genome organization for a coronavirus is 5′-leader-UTR-replicase
(ORF1ab)-spike (S)-envelope (E)-membrane (M)-nucleocapsid (N)-3′UTR-poly
(A) tail. The open reading frames 1a
and 1b, which occupy the first two-thirds of the genome, encode the replicase
polyprotein (pp1ab). The replicase polyprotein self cleaves to form 16 nonstructural
proteins (nsp1–nsp16).[43]
The later reading frames encode the four major structural
proteins: spike, envelope, membrane, and nucleocapsid.[49] Interspersed
between these reading frames are the reading frames for the accessory proteins.
The number of accessory proteins and their function is unique depending on the
specific coronavirus.[43]
Replication cycle
Cell entry

The life cycle of a coronavirus
Infection begins when the viral spike protein attaches to
its complementary host cell receptor. After attachment, a protease of the host cell cleaves and activates the
receptor-attached spike protein. Depending on the host cell protease available,
cleavage and activation allows the virus to enter the host cell by endocytosis or direct fusion of the viral
envelop with the host membrane.[50]
Genome translation
On entry into the host cell, the virus particle is uncoated, and its genome enters the cell cytoplasm. The coronavirus RNA genome has
a 5′ methylated cap and a 3′ polyadenylated tail, which allows it to act like
a messenger RNA and
be directly translated by the host cell's ribosomes. The host ribosomes translate the
initial overlapping open reading frames ORF1a
and ORF1b of the virus genome into two large overlapping polyproteins, pp1a and
pp1ab.[43]

SARS-CoV genome and proteins
The larger polyprotein pp1ab is a result of a -1 ribosomal
frameshift caused by a slippery sequence (UUUAAAC) and a
downstream RNA
pseudoknot at the end of open reading frame ORF1a.[51] The
ribosomal frameshift allows for the continuous translation of ORF1a followed by
ORF1b.[43]
The polyproteins have their own proteases, PLpro (nsp3) and 3CLpro (nsp5), which cleave the
polyproteins at different specific sites. The cleavage of polyprotein pp1ab
yields 16 nonstructural proteins (nsp1 to nsp16). Product proteins include
various replication proteins such as RNA-dependent
RNA polymerase (nsp12), RNA helicase (nsp13), and exoribonuclease (nsp14).[43]
Replicase-transcriptase
Replicase-transcriptase complex
A number of the nonstructural proteins coalesce to form
a multi-protein replicase-transcriptase
complex. The main replicase-transcriptase protein is the RNA-dependent
RNA polymerase (RdRp). It is directly involved in the replication and transcription of
RNA from an RNA strand. The other nonstructural proteins in the complex assist
in the replication and transcription process. The exoribonuclease nonstructural protein,
for instance, provides extra fidelity to replication by providing a proofreading function
which the RNA-dependent RNA polymerase lacks.[52]
Replication – One of the main
functions of the complex is to replicate the viral genome. RdRp directly
mediates the synthesis of
negative-sense genomic RNA from the positive-sense genomic RNA. This is
followed by the replication of positive-sense genomic RNA from the
negative-sense genomic RNA.[43]
Transcription of nested mRNAs

Nested set of subgenomic mRNAs
Transcription – The other
important function of the complex is to transcribe the viral genome. RdRp
directly mediates the synthesis of
negative-sense subgenomic RNA molecules from the positive-sense genomic RNA.
This process is followed by the transcription of these negative-sense
subgenomic RNA molecules to their corresponding positive-sense mRNAs.[43] The
subgenomic mRNAs form a "nested set" which have a common 5'-head
and partially duplicate 3'-end.[53]
Recombination – The
replicase-transcriptase complex is also capable of genetic recombination when
at least two viral genomes are present in the same infected cell.[53] RNA
recombination appears to be a major driving force in determining genetic
variability within a coronavirus species, the capability of a coronavirus
species to jump from one host to another and, infrequently, in determining the
emergence of novel coronaviruses.[54] The
exact mechanism of recombination in coronaviruses is unclear, but likely
involves template switching during genome replication.[54]
Assembly and release
The replicated positive-sense genomic RNA becomes the
genome of the progeny viruses.
The mRNAs are gene transcripts of the last third of the virus genome after the
initial overlapping reading frame. These mRNAs are translated by the host's
ribosomes into the structural proteins and a number of accessory proteins.[43] RNA
translation occurs inside the endoplasmic reticulum.
The viral structural proteins S, E, and M move along the secretory pathway into
the Golgi
intermediate compartment. There, the M proteins
direct most protein-protein interactions required for assembly of viruses
following its binding to the nucleocapsid. Progeny viruses are then
released from the host cell by exocytosis through secretory vesicles.
Once released the viruses can infect other host cells.[55]
Transmission
Infected carriers are able to shed viruses into
the environment. The interaction of the coronavirus spike protein with its
complementary cell receptor is
central in determining the tissue tropism, infectivity, and species range of the released virus.[56][57] Coronaviruses
mainly target epithelial cells.[5] They
are transmitted from one host to another host, depending on the coronavirus
species, by either an aerosol, fomite, or fecal-oral route.[58]
Human coronaviruses infect the epithelial cells of
the respiratory tract,
while animal coronaviruses generally infect the epithelial cells of the digestive tract.[5] SARS coronavirus, for example, infects via an
aerosol route,[59] the
human epithelial cells of the lungs by binding to the angiotensin-converting
enzyme 2 (ACE2) receptor.[60] Transmissible
gastroenteritis coronavirus (TGEV) infects, via a fecal-oral
route,[58] the
pig epithelial cells of the digestive tract by binding to the alanine
aminopeptidase (APN) receptor.[43]
Classification
For a more detailed list of members,
see Coronaviridae.

Phylogenetic tree of coronaviruses
The scientific name for coronavirus is Orthocoronavirinae or Coronavirinae.[2][3][4] Coronaviruses
belong to the family of Coronaviridae, order Nidovirales, and realm Riboviria.[5][6] They
are divided into alphacoronaviruses and betacoronaviruses which infect
mammals – and gammacoronaviruses and deltacoronaviruses, which primarily
infect birds.[61][62]
o Species: Alphacoronavirus
1, Human coronavirus
229E, Human coronavirus
NL63, Miniopterus
bat coronavirus 1, Miniopterus
bat coronavirus HKU8, Porcine
epidemic diarrhea virus, Rhinolophus
bat coronavirus HKU2, Scotophilus
bat coronavirus 512
o Species: Betacoronavirus 1 (Bovine Coronavirus, Human coronavirus
OC43), Hedgehog coronavirus
1, Human coronavirus HKU1, Middle East respiratory syndrome-related coronavirus, Murine coronavirus, Pipistrellus
bat coronavirus HKU5, Rousettus
bat coronavirus HKU9, Severe acute respiratory syndrome-related coronavirus (SARS-CoV, SARS-CoV-2), Tylonycteris
bat coronavirus HKU4
o Species: Avian coronavirus, Beluga whale
coronavirus SW1
·
Genus Deltacoronavirus; type species: Bulbul coronavirus
HKU11
o Species: Bulbul coronavirus
HKU11, Porcine coronavirus HKU15
Origin

Origins of human coronaviruses with possible intermediate hosts
The most recent
common ancestor (MRCA) of all coronaviruses is estimated to
have existed as recently as 8000 BCE,
although some models place the common ancestor as far back as 55 million years
or more, implying long term coevolution with bat and avian species.[63] The
most recent common ancestor of the alphacoronavirus line has been placed at
about 2400 BCE, of the betacoronavirus line at 3300 BCE, of the
gammacoronavirus line at 2800 BCE, and of the deltacoronavirus line at about
3000 BCE. Bats and birds, as warm-blooded flying vertebrates, are an
ideal natural reservoir for
the coronavirus gene pool (with bats the reservoir for alphacoronaviruses
and betacoronavirus – and birds the reservoir for gammacoronaviruses and
deltacoronaviruses). The large number and global range of bat and avian species
that host viruses has enabled extensive evolution and dissemination of
coronaviruses.[64]
Many human coronaviruses have their origin in bats.[65] The
human coronavirus NL63 shared a common ancestor with a bat coronavirus
(ARCoV.2) between 1190 and 1449 CE.[66] The
human coronavirus 229E shared a common ancestor with a bat coronavirus (GhanaGrp1
Bt CoV) between 1686 and 1800 CE.[67] More
recently, alpaca coronavirus and human coronavirus
229E diverged sometime before 1960.[68] MERS-CoV
emerged in humans from bats through the intermediate host of camels.[69] MERS-CoV,
although related to several bat coronavirus species, appears to have diverged
from these several centuries ago.[70] The
most closely related bat coronavirus and SARS-CoV diverged in 1986.[71] A
possible path of evolution of SARS coronavirus and keen bat coronaviruses is
that SARS-related coronaviruses coevolved in bats for a long time. The
ancestors of SARS-CoV first infected leaf-nose bats of the genus Hipposideridae; subsequently, they spread
to horseshoe bats in the species Rhinolophidae, then to Asian palm civets, and finally to humans.[72][73]
Unlike other betacoronaviruses, bovine coronavirus of
the species Betacoronavirus 1 and
subgenus Embecovirus is
thought to have originated in rodents and not in bats.[65][74] In
the 1790s, equine coronavirus diverged from the bovine coronavirus after
a cross-species
jump.[75] Later
in the 1890s, human coronavirus OC43 diverged from bovine coronavirus after another
cross-species spillover event.[76][75] It
is speculated that the flu pandemic of 1890 may
have been caused by this spillover event, and not by the influenza virus, because of the related
timing, neurological symptoms, and unknown causative agent of the pandemic.[77] Besides
causing respiratory infections, human coronavirus OC43 is also suspected of
playing a role in neurological diseases.[78] In
the 1950s, the human coronavirus OC43 began to diverge into its present genotypes.[79] Phylogentically,
mouse hepatitis virus (Murine coronavirus),
which infects the mouse's liver and central
nervous system,[80] is
related to human coronavirus OC43 and bovine coronavirus. Human coronavirus
HKU1, like the aforementioned viruses, also has its origins in rodents.[65]
Infection in humans

Illustration of SARSr-CoV virion
Coronaviruses vary significantly in risk factor. Some can
kill more than 30% of those infected, such as MERS-CoV, and some are relatively harmless,
such as the common cold.[43] Coronaviruses
can cause colds with major symptoms, such as fever,
and a sore throat from
swollen adenoids.[81] Coronaviruses
can cause pneumonia (either
direct viral pneumonia or
secondary bacterial pneumonia)
and bronchitis (either direct viral
bronchitis or secondary bacterial bronchitis).[82] The
human coronavirus discovered in 2003, SARS-CoV, which causes severe
acute respiratory syndrome (SARS), has a unique pathogenesis
because it causes both upper and lower
respiratory tract infections.[82]
Six species of human coronaviruses are known, with one
species subdivided into two different strains, making seven strains of human
coronaviruses altogether.

Seasonal distribution of HCoV-NL63 in Germany shows a preferential
detection from November to March
Four human coronaviruses produce symptoms that are
generally mild:
1.
Human coronavirus
OC43 (HCoV-OC43), β-CoV
2.
Human coronavirus
HKU1 (HCoV-HKU1), β-CoV
3.
Human coronavirus
229E (HCoV-229E), α-CoV
4.
Human coronavirus
NL63 (HCoV-NL63), α-CoV
Three human coronaviruses produce symptoms that are
potentially severe:
1.
Middle East respiratory syndrome-related coronavirus (MERS-CoV),
β-CoV
2.
Severe
acute respiratory syndrome coronavirus (SARS-CoV), β-CoV
3.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),
β-CoV
Common cold
Main article: Common cold
The human coronaviruses HCoV-OC43, HCoV-HKU1, HCoV-229E, and HCoV-NL63 continually circulate in the
human population and produce the generally mild symptoms of the common cold in adults and children
worldwide.[83] These
coronaviruses cause about 15% of common colds,[84] while
40 to 50% of colds are caused by rhinoviruses.[85] The
four mild coronaviruses have a seasonal incidence occurring in the winter
months in temperate climates.[86][87] There
is no preponderance in any season in tropical climates.[88]
Severe acute respiratory syndrome (SARS)
Main article: Severe
acute respiratory syndrome
|
Characteristics of
zoonotic coronavirus strains
MERS-CoV, SARS-CoV, SARS-CoV-2, and related diseases |
|||
|
Disease
|
|||
|
Outbreaks
|
|||
|
Epidemiology
|
|||
|
Date of first
identified case |
June
2012 |
November
2002 |
|
|
Location of first
identified case |
Jeddah,
Saudi Arabia |
Shunde,
China |
Wuhan,
China |
|
Age average
|
56
|
||
|
Sex ratio (M:F)
|
3.3:1
|
||
|
Confirmed cases
|
2494
|
||
|
Deaths
|
858
|
||
|
Case fatality rate
|
37%
|
9.2%
|
|
|
Symptoms
|
|||
|
Fever
|
98%
|
99–100%
|
|
|
Dry cough
|
47%
|
29–75%
|
|
|
72%
|
40–42%
|
||
|
26%
|
20–25%
|
||
|
Sore throat
|
21%
|
13–25%
|
|
|
Ventilatory use
|
14–20%
|
||
|
Notes
·
v
·
t
·
e
|
|||
In 2003, following the outbreak of severe acute
respiratory syndrome (SARS) which had begun the prior year in Asia, and
secondary cases elsewhere in the world, the World Health
Organization (WHO) issued a press release stating that a novel
coronavirus identified by a number of laboratories was the causative agent for
SARS. The virus was officially named the SARS coronavirus (SARS-CoV). More than
8,000 people were infected, about ten percent of whom died.[60]
Middle East respiratory syndrome (MERS)
Main article: Middle
East respiratory syndrome
In September 2012, a new type of coronavirus was
identified, initially called Novel Coronavirus 2012, and now officially named
Middle East respiratory syndrome coronavirus (MERS-CoV).[98][99] The
World Health Organization issued a global alert soon after.[100] The
WHO update on 28 September 2012 said the virus did not seem to pass easily from
person to person.[101] However,
on 12 May 2013, a case of human-to-human
transmission in France was confirmed by the French Ministry of
Social Affairs and Health.[102] In
addition, cases of human-to-human transmission were reported by the Ministry of
Health in Tunisia. Two confirmed cases involved people
who seemed to have caught the disease from their late father, who became ill
after a visit to Qatar and Saudi Arabia. Despite this, it appears the virus had
trouble spreading from human to human, as most individuals who are infected do
not transmit the virus.[103] By
30 October 2013, there were 124 cases and 52 deaths in Saudi Arabia.[104]
After the Dutch Erasmus Medical Centre sequenced the
virus, the virus was given a new name, Human Coronavirus—Erasmus Medical Centre
(HCoV-EMC). The final name for the virus is Middle East respiratory syndrome
coronavirus (MERS-CoV). The only U.S. cases (both survived) were recorded in
May 2014.[105]
In May 2015, an outbreak of MERS-CoV occurred in
the Republic of Korea,
when a man who had traveled to the Middle East, visited four hospitals in the
Seoul area to treat his illness. This caused one of the largest outbreaks of
MERS-CoV outside the Middle East.[106] As
of December 2019, 2,468 cases of MERS-CoV infection had been confirmed by
laboratory tests, 851 of which were fatal, a mortality rate of approximately 34.5%.[107]
Coronavirus disease 2019 (COVID-19)
Main article: Coronavirus
disease 2019
In December 2019, a pneumonia outbreak was reported
in Wuhan, China.[108] On
31 December 2019, the outbreak was traced to a novel strain of coronavirus,[109] which
was given the interim name 2019-nCoV by the World Health
Organization (WHO),[110][111][112] later
renamed SARS-CoV-2 by
the International
Committee on Taxonomy of Viruses.
As of 6 July 2020, there have been at least 535,027[94] confirmed
deaths and more than 11,483,400[94] confirmed
cases in the COVID-19 pandemic.
The Wuhan strain has been identified as a new strain of Betacoronavirus from group 2B with
approximately 70% genetic similarity to the SARS-CoV.[113] The
virus has a 96% similarity to a bat coronavirus, so it is widely suspected to
originate from bats as well.[114][115] The
pandemic has resulted in travel restrictions and nationwide lockdowns in many
countries.
Infection in animals
Coronaviruses have been recognized as causing
pathological conditions in veterinary medicine since
the 1930s.[17] They
infect a range of animals including swine, cattle, horses, camels, cats, dogs,
rodents, birds and bats.[116] The
majority of animal related coronaviruses infect the intestinal tract and
are transmitted by a fecal-oral route.[117] Significant
research efforts have been focused on elucidating the viral pathogenesis of
these animal coronaviruses, especially by virologists interested in veterinary
and zoonotic diseases.[118]
Farm animals
Coronaviruses infect domesticated birds.[119] Infectious
bronchitis virus (IBV), a type of coronavirus, causes avian
infectious bronchitis.[120] The
virus is of concern to the poultry industry because of the high
mortality from infection, its rapid spread, and affect on production.[116] The
virus affects both meat production and egg production and causes substantial
economic loss.[121] In
chickens, infectious bronchitis virus targets not only the respiratory tract
but also the urogenital tract.
The virus can spread to different organs throughout the chicken.[120] The
virus is transmitted by aersol and food contaminated by feces. Different vaccines against IBV exist and have
helped to limit the spread of the virus and its variants.[116] Infectious
bronchitis virus is one of a number of strains of the species Avian coronavirus.[122] Another
strain of avian coronavirus is turkey coronavirus (TCV)
which causes enteritis in turkeys.[116]
Coronaviruses also affect other branches of animal husbandry such as pig farming and the cattle raising.[116] Swine
acute diarrhea syndrome coronavirus (SADS-CoV), which is
related to bat
coronavirus HKU2, causes diarrhea in pigs.[123] Porcine
epidemic diarrhea virus (PEDV) is a coronavirus that has
recently emerged and similarly causes diarrhea in pigs.[124] Transmissible
gastroenteritis virus (TGEV), which is a member of the
species Alphacoronavirus 1,[125] is
another coronavirus that causes diarrhea in young pigs.[126][127] In
the cattle industry bovine coronavirus (BCV),
which is a member of the species Betacoronavirus 1 and related to
HCoV-OC43,[128] is
responsible for severe profuse enteritis in young calves.[116]
Domestic pets
Coronaviruses infect domestic pets such as cats, dogs,
and ferrets.[119] There
are two forms of feline coronavirus which
are both members of the species Alphacoronavirus 1.[125] Feline
enteric coronavirus is a pathogen of minor clinical significance, but spontaneous mutation of this virus can result
in feline
infectious peritonitis (FIP), a disease with high mortality.[116] There
are two different coronaviruses that infect dogs. Canine coronavirus (CCoV),
which is a member of the species Alphacoronavirus 1,[125] causes
mild gastrointestinal disease.[116] Canine respiratory
coronavirus (CRCoV), which is a member of the species Betacoronavirus 1 and related to HCoV-OC43,[128] cause
respiratory disease.[116] Similarly,
there are two types of coronavirus that infect ferrets.[129] Ferret enteric
coronavirus causes a gastrointestinal syndrome known as
epizootic catarrhal enteritis (ECE), and a more lethal systemic version of the
virus (like FIP in cats) known as ferret systemic coronavirus (FSC).[130][131]
Laboratory animals
Coronaviruses infect laboratory animals.[116] Mouse
hepatitis virus (MHV), which is a member of the species Murine coronavirus,[132] causes
an epidemic murine illness with high mortality,
especially among colonies of laboratory mice.[133] Prior
to the discovery of SARS-CoV, MHV was the best-studied coronavirus both in vivo and in vitro as well as at the molecular
level. Some strains of MHV cause a progressive demyelinating
encephalitis in mice which has been used as a murine model
for multiple sclerosis.[118] Sialodacryoadenitis virus (SDAV), which
is a strain of the species Murine coronavirus,[132] is
highly infectious coronavirus of laboratory rats, which can be transmitted
between individuals by direct contact and indirectly by aerosol. Acute
infections have high morbidity and tropism for the salivary, lachrymal
and harderian glands.[134] Rabbit
enteric coronavirus causes acute gastrointestinal disease and diarrhea in
young European rabbits.[116] Mortality
rates are high.[135]
Prevention and treatment
There are no vaccines or antiviral drugs to prevent or treat human
coronavirus infections. Treatment is only supportive. A number of antivirial targets have been identified
such as viral proteases, polymerases, and entry proteins. Drugs are in
development which target these proteins and the different steps
of viral replication. A number of vaccines using different
methods are also under development for different human coronaviruses.[43]
There are no antiviral drugs to treat animal
coronaviruses.[citation needed] Vaccines are available for IBV, TGEV, and Canine CoV, although their
effectiveness is limited. In the case of outbreaks of highly contagious animal
coronaviruses, such as PEDV, measures such as destruction of entire herds of pigs may
be used to prevent transmission to other herds.[43]
**
This is simply a few sites I pulled information from and EVERY site it is EASY
to see that the true cause of death comes from being put on a ventilator….
Which hidden camera whistleblowers are confirming every day – that ventilator
settings and the medications are what is truly killing people…..
Now
YOU are armed with the knowledge of what a corona virus is, how it behaves and
how YOU can handle it….. BTW corona virus is also VERY well known and listed on
the back of a Lysol can….. You know it as “the common cold”
My
dear friends YOU have been duped by mainstream media and moron so called
experts….
Please
use this information wisely and stop allowing mainstream media to force you to
live in fear….
No comments:
Post a Comment
Your message has been sent to the moderator for approval and shall appear very soon!